The Kidney Project
The goal of Kidney Project is to overcome scarcity and engineer a limitless supply of implantable artificial kidneys to improve the lives of patients with renal failure.

A long-term effort by multiple universities, including Vanderbilt University and University of California–San Francisco, The Kidney Project envisions a better future for people facing kidney failure, without dialysis, without pumps, tubes, or immunosuppressive drugs.
PROBLEM
Sickness and scarcity
Half a million Americans and two million people worldwide feel sick every day because they have severe kidney disease. Ideally, every person suffering from kidney failure would be able to receive a healthy kidney through an altruistic living donor or a deceased donor. But at any given time, there are five times as many people waiting for a kidney as there are available kidneys for transplantation. According to the United Network for Organ Sharing, nearly 90,000 people in the United States are waiting for a kidney transplant, and 11 people die every day while waiting.
Those unable to receive a kidney transplant face an earlier death or must choose some form of dialysis, which can be burdensome and only replaces a small fraction of the function of a healthy kidney. Kidney transplant recipients can live a longer, more normal life than they would with dialysis treatment.
Treating patients with hemodialysis is costing Americans a fortune and leaving too many people sick. The Kidney Project wants to change that.
SOLUTION
An implantable artificial kidney
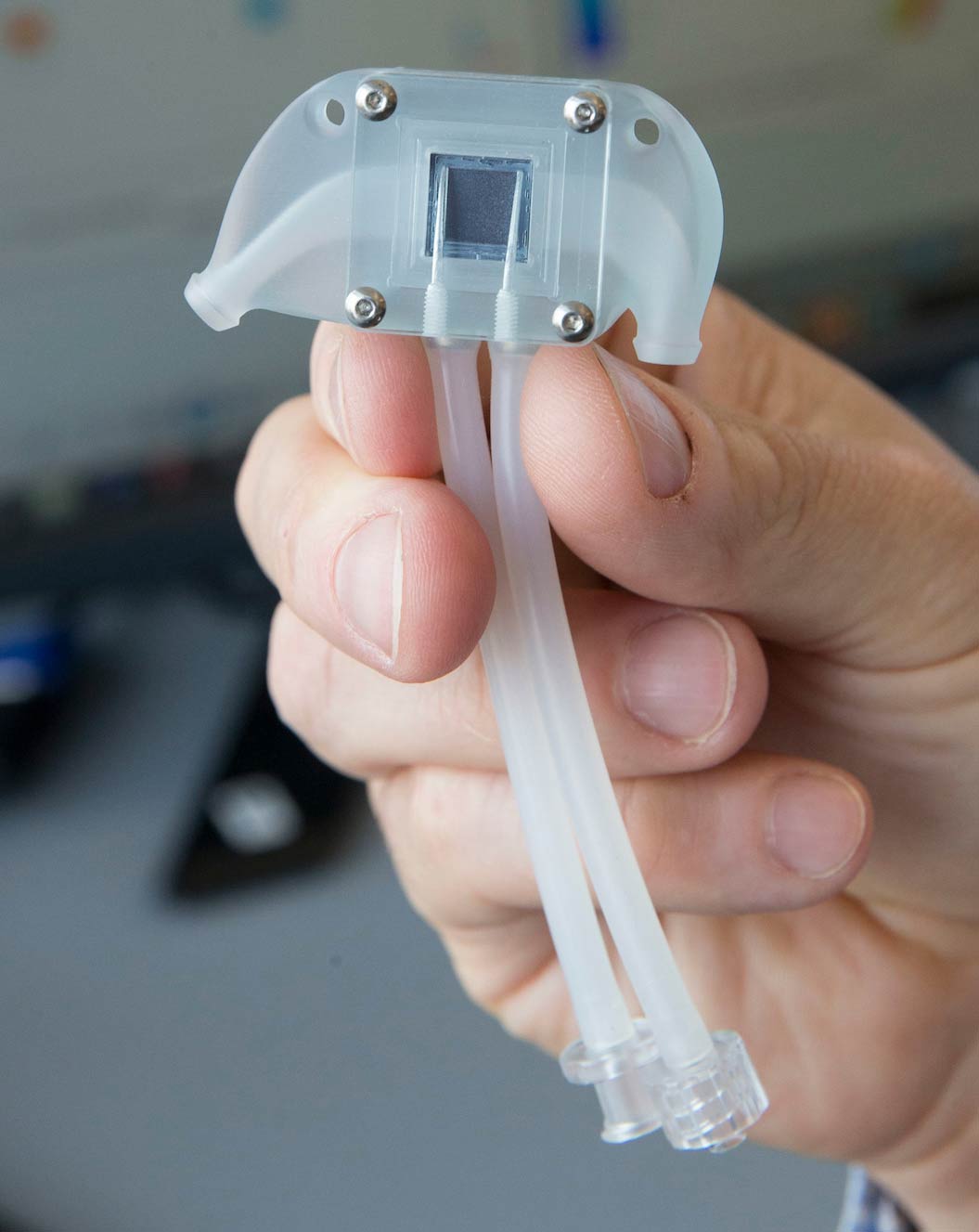
Right now, transplant is limited by a scarcity of donor organs. To solve this problem, researchers with The Kidney Project are working to create an implantable artificial kidney.
Our design copies key features of a healthy, functioning kidney and is modeled on the body’s own strategy for cleaning the blood. The implantable bioartificial kidney combines silicon nanotechnology with tissues from human kidney cells, featuring an artificial filtration unit to replace the cells damaged in end-stage renal failure.
Our goal is a mass-produced universal donor kidney so that every patient with kidney failure can enjoy the benefits of transplant.

Donate
to support the research and development of an artificial implantable kidney
Dr. Bill Fissell's goal is a mass-produced universal donor kidney so that every patient with kidney failure can enjoy the benefits of transplant. This dream is within reach: some of the technology is being reviewed by the Food and Drug Administration for clinical trials. As Dr. Fissell’s work grows from science to engineering to development and testing, his lab is ever more dependent on the generosity of patients like you to bring this dream from the lab bench to clinical trials.
Resources

University of California
San Francisco – The Kidney Project
United Network for Organ Sharing