CGC+ CD4+ T cells are present in the coronary arteries of persons living with HIV
CMV-specific CD4+ T cells are CD57+ GPR56+ CX3CR1+ (CGC+) and associated with carotid plaque burden measured by carotid-B-ultrasound and subclinical atherosclerosis measured by computed tomography angiography. We have also defined the CMV specificity of peripheral CGC+ CD4+ T cells using tetramers.
The goal is to broadly characterize the CMV-specificity of CGC+ T cells and establish whether they are involved in the causal pathway for the development of cardiometabolic disease.
CX3CR1+ GPR56+ CD57+ CD4+ T cells are present in coronary arteries and aorta
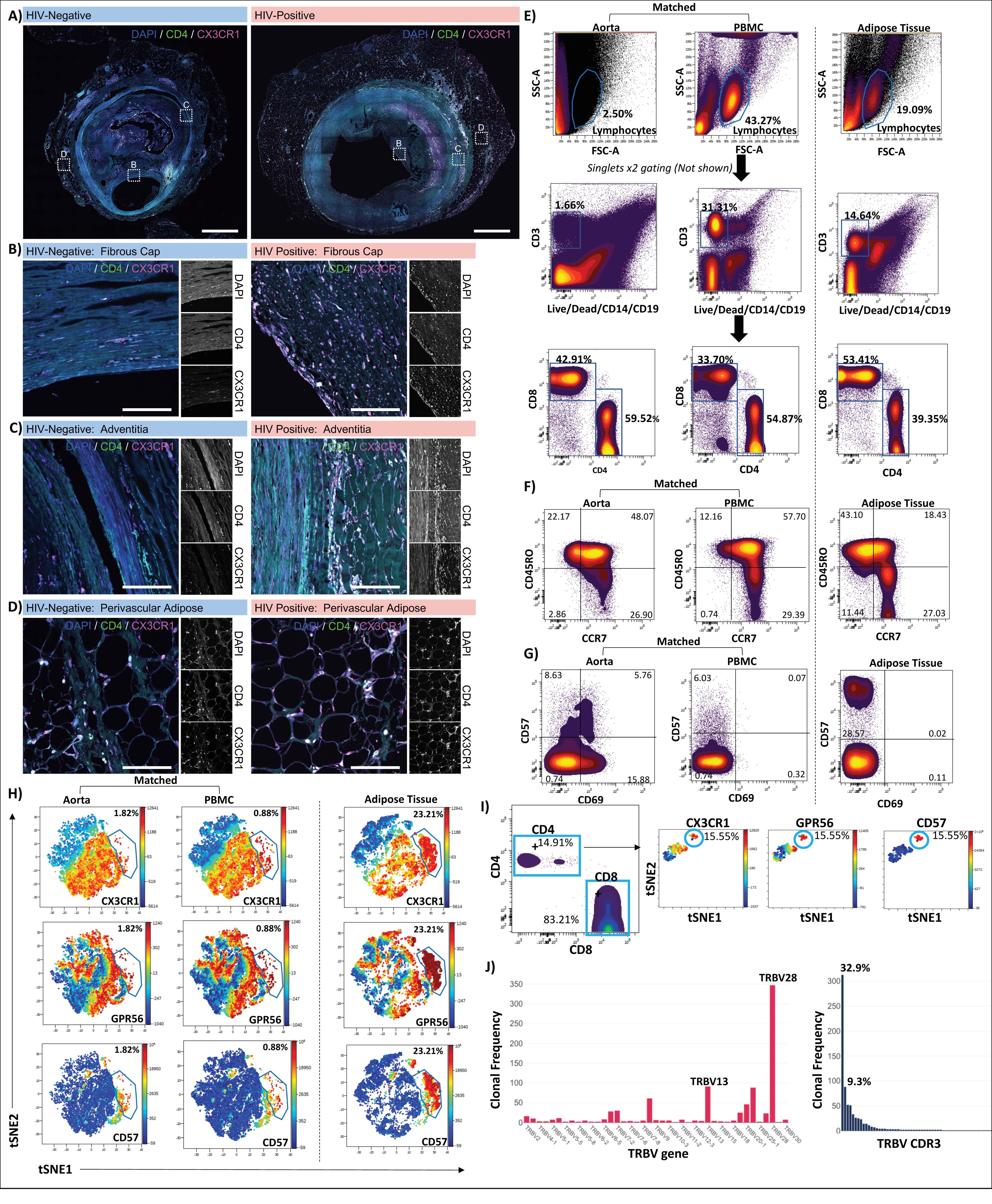
Low magnification confocal images of whole coronary plaques from HIV-negative (left) and HIV-positive (right) persons labeled with DAPI (blue), anti-CD4 (green), and anti-CX3CR1 (magenta), Scale bars 1000 µm (A). Enlarged images of the intima/fibrous cap (B), adventitia (C), and perivascular adipose (D), scale bars 500 µm.
Single cells isolated from the aorta of an HIV-negative individual were stained with the 12-antibody panel, including CX3CR1, GPR56, and CD57. Peripheral blood mononuclear cells (PBMCs) from the same person and subcutaneous adipose tissue from an HIV-positive participant as a positive control for tissue C-G-C+ CD4+ T cells were stained simultaneously. Lymphocytes, single cells, CD3+ live, CD4+ , and CD8+ T cells were gated as shown (E). T-cell memory populations were gated based on CCR7 and CD45RO co-expression (F).
Two-dimensional plots show expression of CD57 and CD69 (G). viSNE plots show C-G-C+ CD4+ T cells from the aorta and PBMCs of HIV-negative donor and HIV-positive subcutaneous adipose tissue (H). C-G-C+ CD4+ T cells were identified in a second HIV-negative aorta (I). Out of 949 CD3+ T cells isolated and sequenced from the aorta of the second donor, 240 clones were identified. The T-cell receptor (TCR) β V gene and CDR3 clonal frequencies are shown (J).
Read more:
CGC+ CD4+ T cells are increased in persons with liver disease, and diabetes in people living with HIV
Individuals with HIV and diabetes have higher levels of CD4+ T cells that express CD57, GPR56, and CX3CR1 (CGC+) in their adipose tissue and peripheral blood. A high proportion of CGC+ CD4+ T cells in the peripheral blood is linked to carotid plaque burden. We are currently conducting studies to determine the antigens responsible for maintaining CGC+ T cells and the role of these immune cells in tissue.
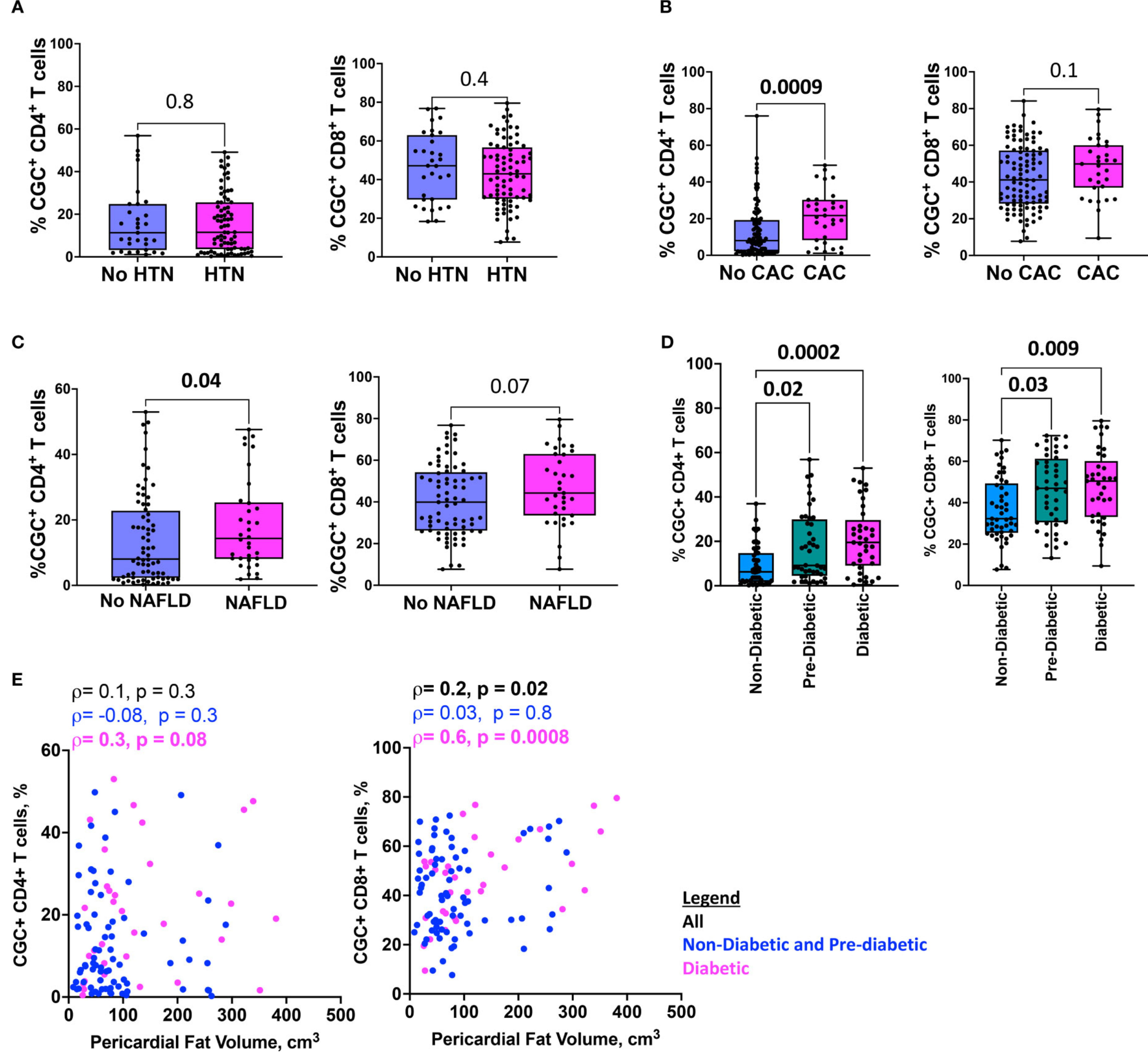
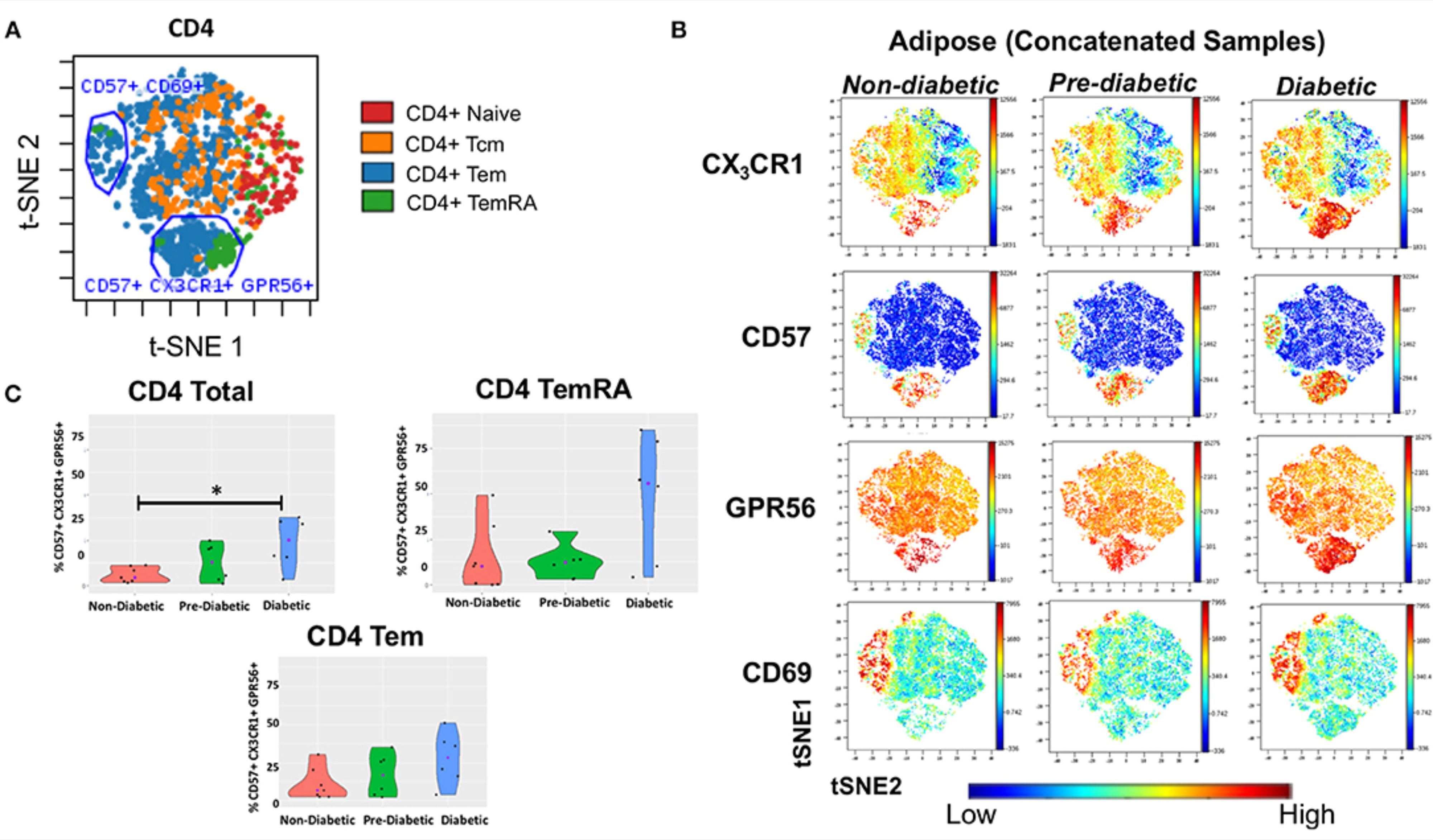
Individuals with HIV and diabetes have higher levels of CD4+ T cells that express CD57, GPR56, and CX3CR1 (CGC+) in their adipose tissue and peripheral blood
Image description: CD4+ T cells co-expressing CD57, CX3CR1, and GPR56 in subcutaneous adipose tissue increase with progressive glucose intolerance. viSNE plots were generated in Cytobank to identify groups of cells that differ between non-diabetic, pre-diabetic, and diabetic categories.
(A) Clusters of CD4+, TNaive, TEM, TCM, and TEMRA cells from subcutaneous adipose tissue (SAT). (B) Concatenated viSNE plots of non-diabetic, pre-diabetic, and diabetic PLWH showing clusters of cells expressing CX3CR1, CD57, GPR56, and CD69. (C) Violin plots showing the percentage of total CD4+, TEM, and TEMRA cells co-expressing CD57, CX3CR1, and GPR56. Mann-Whitney test was used to analyze differences between metabolic groups; *P < 0.05.
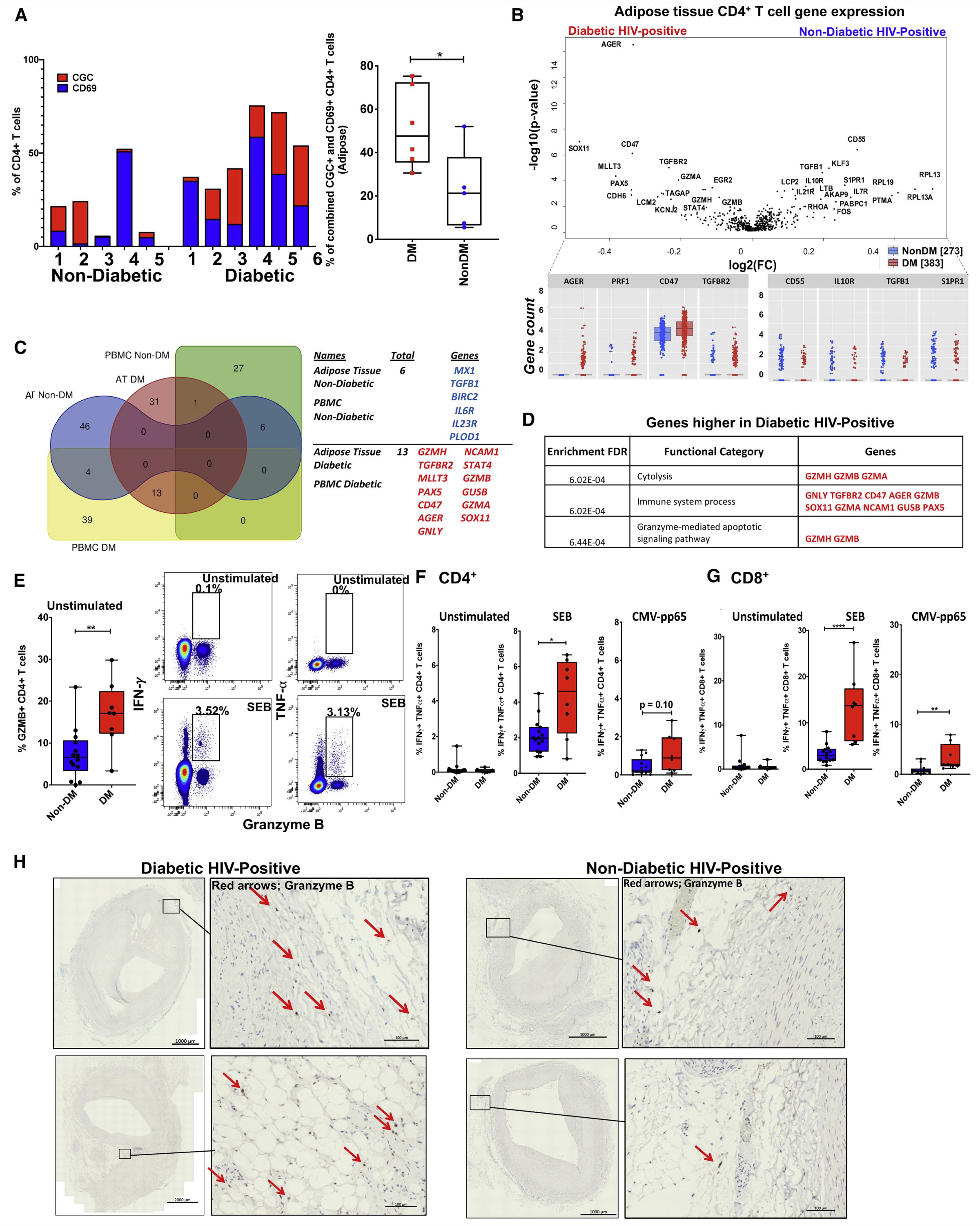
Single-cell analysis shows that adipose tissue of persons with both HIV and diabetes is enriched for clonal, cytotoxic, and CMV-specific CD4+ T cells
Wanjalla et al. demonstrate that adipose tissue in persons with HIV and diabetes includes a large proportion of clonally expanded, inflammatory, and frequently CMV-specific CX3CR1+ GPR56+ CD57+(C-G-C+) CD4+ T cells. These cells may contribute to the altered adipocyte function and elevated risk of metabolic disease observed among persons with HIV.
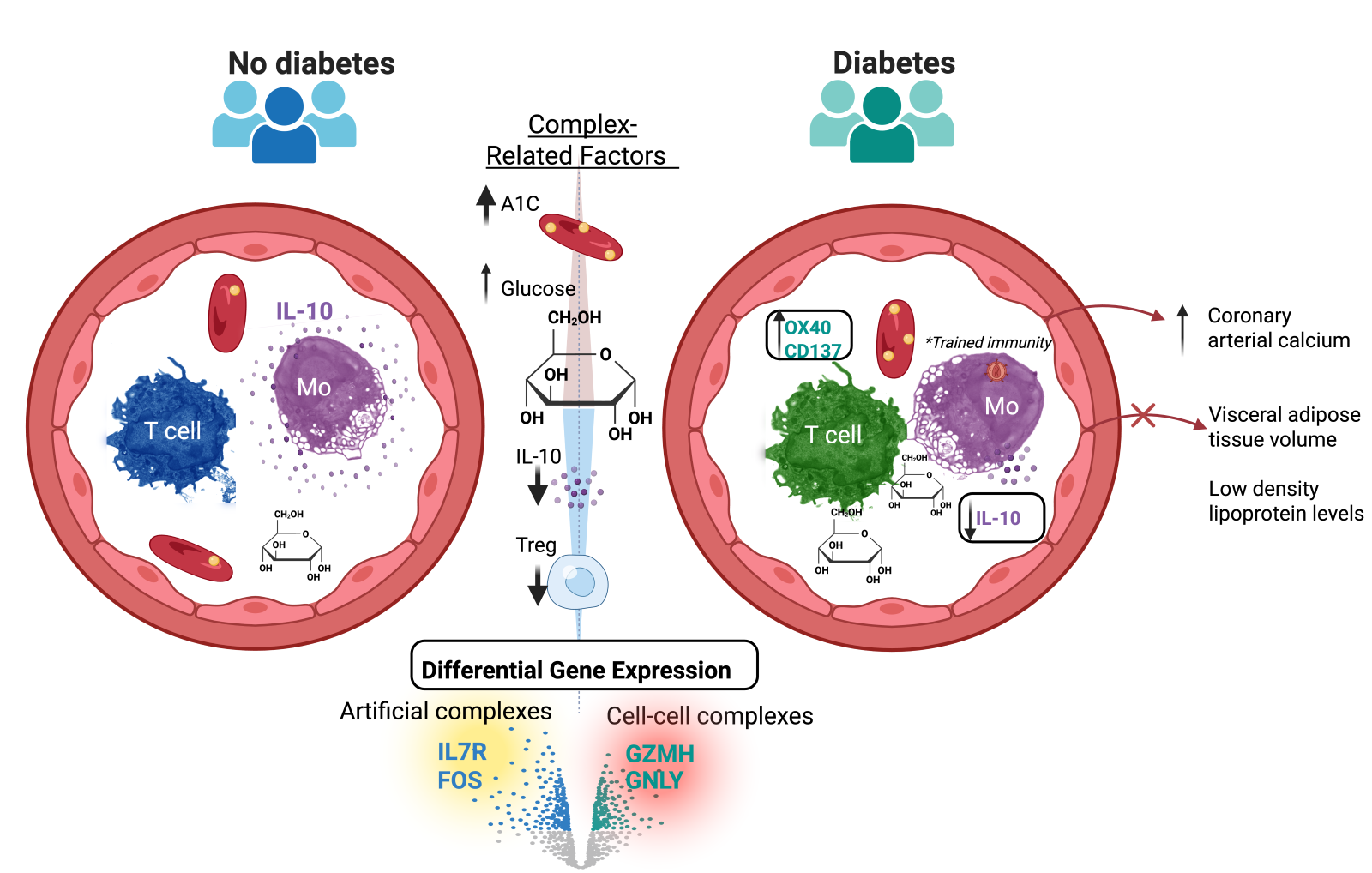
CD3+ T-cell: CD14+ monocyte complexes are dynamic and increased with HIV and glucose intolerance
Obare et al. show that circulating CD3⁺ T-cell:CD14⁺ monocyte complexes are dynamic, biologically relevant, and increased in people with HIV and glucose intolerance.
These complexes form stable immune synapses, are enriched for activated and proinflammatory T cells (including Th17 subsets), and contain more HIV copies than singlet T cells or monocytes. Their abundance correlates with higher fasting glucose and hemoglobin A1C and lower IL-10 and regulatory T cells, suggesting they contribute to systemic inflammation, viral persistence, and cardiometabolic disease risk in persons with HIV.